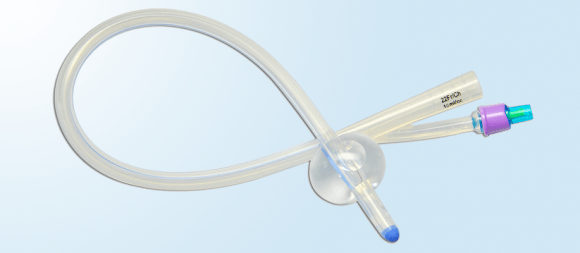
A balloon enema program is very much like a cone enema program, except the enema is delivered through a latex-free foley catheter (usually 24fr) hooked to a gravity feeding bag instead of through the cone irrigation kit. The catheter, inserted in the rectum and inflated, prevents the water/solution from coming back out immediately.
How it’s Done
Many of the bowel bootcamps use balloon enemas instead of cones for patients with various diagnoses, not just Spina Bifida. So most people using the balloon enema have already received an extensive training and receive supplies through a medical supply company. But as a brief overview of the procedure: a child usually lays on the floor (on a mat or towel) preferably with bottom raised in the air, and a caregiver inserts the catheter into the rectum about 4 inches, inflates the balloon, and opens the valve on the gravity bag for fluid to start flowing into the rectum. (Less commonly, someone instead injects the solution into the catheter with one or more 60+ml syringes instead of using a gravity bag.) It is best to have the child lay down for about 10 minutes before transferring to the toilet where the balloon can be deflated. Just as with the cone enema, it usually takes about 45 minutes to fully empty. Besides the administration, most of the other principles (recipe, when, how often, FAQ’s) of the cone enema program apply here as well.
FAQ: Why does the balloon keep popping out?
The balloon enema works great at bowel bootcamps for kids with all sorts of bowel issues, but Spina Bifida adds the additional challenge of low muscle tone to hold in the balloon. It’s very common to find that the balloon pops out when water starts filling the colon. However, there are ways to fix the problem. Although it is generally advised to inflate a 24fr catheter no bigger than 30cc, many people find that they can and must inflate the balloon much higher–to 40, 50, 60, 70 or even 80 cc. Some also have luck inflating the balloon with water instead of air to keep it from popping out of a loose rectum. If the balloon has been working for awhile but it suddenly starts popping out, consider whether the child is constipated. If these tricks fail, some will simply switch to a cone enema kit.
FAQ: Which is better, cone enema or balloon enema?
For the most part, neither is better or worse, but there are a few pros and cons of each. If you go to a bowel bootcamp, you will probably use the balloon enema simply because that is what they usually use. They will train you and set you up with a supply company, and supplies can be billed to insurance. The balloon enema can potentially be less messy than the cone enema if a child has the ability to independently transfer from floor to toilet because the balloon can typically hold during the transfer and be deflated once the child is on the toilet. In contrast, the person administering the cone enema would have to hold the cone in with their hand during any transfer, and even if the whole process is done on the toilet, removing the cone can be messier than deflating and removing the balloon.
If you do not have access to a bowel bootcamp or knowledgeable bowel doctor and must start the process on your own (with the help of the Cone Enema Guide and the Bowel Management for Spina Bifida Facebook Group), cone enema supplies are much easier to purchase online inexpensively without a prescription. The other main benefit of the cone enema is that it can more easily administered on the toilet since someone’s hand is holding it in against gravity. Although some people have success administering the balloon enema on the toilet, the balloon often pops out due to low muscle tone plus gravity plus pressure from the fluid in the rectum.
Both cone and balloon enema programs can be excellent bowel management programs for children around age 3 and up to help prevent constipation and promote continence. Major considerations are that they only clean out the descending colon, and that they are difficult (although not impossible for those with fewer mobility and flexibility deficits) for an older child, teen, or adult to administer them independently. When it is time to start thinking about independence with a bowel program, consider the Peristeen or the MACE or Cecostomy.
Next: Peristeen
